By Mike Kocsis | 7 minutes read | Last updated: May 2, 2025 Categories: Testosterone
Medically Reviewed by Dr. George Touliatos
Human chorionic gonadotropin (hCG), often referred to as the ‘pregnancy hormone,’ is a naturally occurring hormone essential for reproductive processes.
hCG supports egg production in females and sperm production in males. Additionally, it is sometimes used medically to stimulate these functions in individuals.
What is hCG?
Human chorionic gonadotropin (hCG) is a hormone primarily produced in the female placenta. Its primary function is to stimulate ovulation and maintain fertility.
HCG was first discovered in the early 1900s, and since then much research has been done on this fascinating hormone.
Scientists realised that injections of hCG could help improve fertility in women who were unable to get pregnant.
Later on, researchers found out that hCG was also a suitable treatment for hypogonadism (low testosterone levels) in men. This is because it can help stimulate endogenous testosterone (natural testosterone) production.
hCG is sold under various brand names, including Pregnyl, Profasi HP, Novarel, and Ovidrel.

How Does hCG Work: Mechanism of Action
In men, the testosterone production process begins when the hypothalamus in the brain detects that the body needs testosterone.
After this, it sends a signal to the anterior pituitary gland to secrete gonadotropin hormones: luteinising hormone (LH) and follicle-stimulating hormone (FSH).
These hormones stimulate sperm and testosterone production in the testes.
The process will start over again once the hypothalamus detects the body needs testosterone. This is known as the HPTA (hypothalamus pituitary axis) feedback loop.
hCG closely resembles the molecular structure of LH. As a result, hCG mimics the action of LH in the male body, leading to sperm production (spermatogenesis) and testosterone production.
The primary difference between LH and hCG is their half-life, i.e. the time it circulates in the body.
LH has a circulating half-life of around 25-30 minutes.
Whereas HCG has a half-life of around 37 hours, making it an ideal prescription for hormone replacement therapy… after all, you definitely don’t want to be injecting every 30 minutes!
What is hCG Used for in Men?
A doctor can prescribe hCG to men for multiple reasons, such as:
- Increase serum testosterone levels
- Manage symptoms of male hypogonadism
- Boost sexual function
- Restore fertility or sperm production in men on testosterone
- Stimulate the descent of the testicles into the scrotum in children with undescended testicles
- Reverse anabolic steroid side effects in bodybuilders who use testosterone to increase muscular strength
How Do You Use hCG?
In men, hCG can raise endogenous (natural) levels of testosterone.
By comparison, testosterone replacement therapy (TRT) uses exogenous (i.e. not made in the body) testosterone, which in turn shuts down the body’s own natural supply.
This is because the body detects that there is enough testosterone in the bloodstream and subsequently stops producing its own.
This is where hCG comes to help men on TRT who want to boost their endogenous testosterone production.
For men using hCG as part of hormone replacement therapy (HRT), there are two options:
Combining hCG with TRT
The first treatment option is to use hCG alongside TRT. This treatment option is ideal for men who want to maintain fertility while experiencing the benefits of TRT.
Men who aren’t concerned about fertility may also choose this option because exogenous testosterone tends to shrink the testes, whereas maintaining fertility through hCG will help maintain normal testicle size.
In certain instances however, using hCG alongside TRT may require an aromatase inhibitor (AI) in order to manage oestrogenic side effects such as bloating and water retention.
hCG monotherapy
The second treatment option for hCG is monotherapy. That means using hCG only to raise intratesticular (i.e. natural) testosterone levels without exogenous testosterone (TRT).
This option works well for men who prefer to maintain their natural testosterone levels only. It may also suit someone who wants to remain on one form of medication only.
In most cases, only men who have secondary or hypogonadotropic hypogonadism (low testosterone) will respond well to hCG as a monotherapy.
Secondary hypogonadism is where there is a problem in the hypothalamus or pituitary area of the brain. These parts of the brain are responsible for sending a signal to the testes to produce testosterone.
Can You Use hCG Monotherapy for Primary Hypogonadism?
In primary hypogonadism, the brain functions normally and sends a signal to the testes to produce testosterone.
However here, the testes fail to respond to this signal and produce testosterone. This generally indicates that there is a problem with the reproductive tissue in the testes.
As mentioned, hCG acts in a similar manner to LH in the male body. If the testes do not respond to a strong LH signal, it is unlikely they will respond to hCG.
What Does the Latest Research Say about the Effectiveness of hCG?
Research on hCG’s ability to both maintain fertility and boost testosterone levels is promising.
In a 2022 study published in The Journal of Sexual Medicine, 31 men with hypogonadal or low testosterone symptoms received hCG monotherapy. Their weekly hCG dosage was 1500 IU.
By the end of the research, they noticed a significant improvement in their testosterone levels, erectile dysfunction (ED), low libido and low energy.
According to another research, hCG restores fertility in up to 70% of patients with hypogonadotropic hypogonadism (i.e. secondary hypogonadism).
A 2018 study indicates that hCG can help men with low testosterone manage infertility. It increases testosterone and sperm production whether used alone or in combination with TRT.
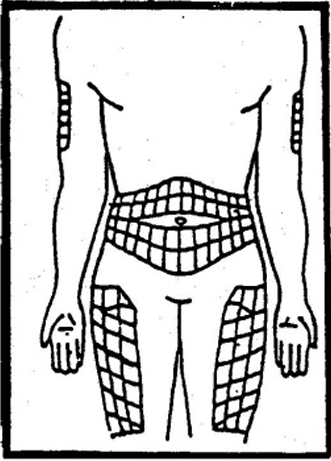
How is hCG Administered?
hCG must be injected subcutaneously (i.e. into fat tissue) in the stomach, upper arms, and front or outer thigh.
If hCG is used with TRT, then the hCG injections would typically be separate on separate days to the testosterone injections.
Anecdotally, there are some individuals who inject both hCG and testosterone at the same time. In theory, this is to improve efficiency.
However, in practice, it is never a good idea to combine two different pharmaceutical substances in such a manner.
hCG comes in a dry powder form and must be mixed with bacteriostatic water before being injected.
Draw the correct amount of bacteriostatic water into a syringe and add it to the vial containing the hCG powder. Once mixed, the hCG solution is drawn into the syringe and is ready for injection.
Hold a 1- to 2-inch fold of skin between your fingers, then insert the needle at a 90-degree angle into the subcutaneous fat, ensuring it does not go too deep.
Slowly push the plunger of the syringe to inject hCG. Once it is done, remove and dispose of the syringe. Apply minor pressure on the injection site to prevent any minor bleeding.
How Do You Dose hCG?
The dose of hCG depends on the patient’s goals – whether they want to maintain fertility or simply maintain testicular size. This typically ranges from 250- 500 IU three times per week.
As with testosterone replacement therapy, there are no standard doses of hCG, because we are biochemically unique. The patient would usually start out on a small, manageable dose of hCG.
From there, it is a case of experimentation and treatment monitoring via blood tests and symptom resolution. Then the doctor can adjust the dose based on feedback from the patient.
Common Injection Protocol (hCG alongside TRT)
- Monday – Testosterone injection of 100mg of sustanon
- Tuesday – hCG injection of 500iu of pregnyl
- Wednesday – non-injection day
- Thursday – hCG injection of 500iu of pregnyl
- Friday – Testosterone injection of 100mg of sustanon
- Saturday – hCG injection of 500iu of pregnyl
- Sunday – non-injection day
The injection protocol for hCG as a monotherapy would be similar to the above. With monotherapy however, there would obviously be no testosterone injections.
The dose for hCG monotherapy is case-dependent. But for most men, this will be anywhere from 1500- 3000 IU per week.
What are the Side Effects of hCG?
Although hCG is a safe and effective solution to increasing testosterone, it may still cause side effects such as:
- Acne
- Headache
- Mood changes
- Lack of energy
- Breast tenderness (due to elevated oestrogen levels)
- Breast enlargement (gynecomastia)
- Stomach pain
- Pain at the injection site
Some of these go away on their own without requiring medical attention. But others may persist or worsen and should be discussed with a healthcare provider.
They may change your dose, prescribe another medication to tackle side effects or even change the complete treatment plan based on how your body reacts to it.
Where Can You Buy hCG in the UK?
hCG has been used for many years to help stimulate fertility in women. However, it is still relatively new as a hormone therapy treatment for men.
The only way you can legally obtain hCG in the UK is through a doctor’s prescription – whether that is private or via the NHS.
Many doctors have little to no experience with hCG in the UK. As a result, it is unlikely you will find an NHS doctor willing to prescribe it as an adjunct to testosterone replacement therapy.
And what is more, highly unlikely you will find a doctor willing to prescribe hCG as a monotherapy in the UK.
At Balance My Hormones, we offer hCG alongside TRT when needed – especially in cases where preserving fertility or preventing testicular shrinkage is a concern.
More hCG Related Questions
Is hCG legal in the UK?
HCG is a legal medication in the UK but is classified as a prescription-only medication. This means you can only obtain it with a doctor’s prescription for approved medical uses such as male fertility treatments.
How long for hCG to work in men?
The time period hCG needs to show results depends on your individual condition and treatment goals.
Studies show that hCG increases plasma testosterone levels in 2 to 4 hours after injection administration. But you may start seeing noticeable results only after a few months.
How long to take hCG for men?
HCG treatment duration is governed by your health condition, goals and how your body responds to it.
In most cases, it is taken for at least a full 3 months. But therapy can take years to show full effects, depending on your needs. Discuss your case with your healthcare provider to learn how long you will need to take hCG for your individual case.
Final Thoughts
hCG is an excellent treatment option for a person looking to increase their testosterone levels.
Nevertheless, as with testosterone, using hCG may require some iteration and experimentation until you find the correct dose for your treatment.
Your suitability for hCG will first depend on your current situation. To begin with – do you have low testosterone? If you have low testosterone, do you have primary or secondary hypogonadism? As this will determine whether hCG is right for you or not.
It also depends on what you want to achieve. Do you want to maintain your fertility and raise your testosterone levels? Or perhaps you are not concerned about fertility, and only want to boost your testosterone levels?
To learn more details about hCG and whether it’s the right choice for you, get in contact with us today.
Our experienced team of doctors, some of whom are on hCG themselves, can go through your treatment options with you with no obligation.
References
- Rajkanna, J., Tariq, S. and Oyibo, S.O., 2016. Successful fertility treatment with gonadotrophin therapy for male hypogonadotrophic hypogonadism. Endocrinology, Diabetes & Metabolism Case Reports, 2016(1).
- Madhusoodanan, V., Patel, P., Lima, T.F.N., Gondokusumo, J., Lo, E., Thirumavalavan, N., Lipshultz, L.I. and Ramasamy, R., 2019. Human Chorionic Gonadotropin monotherapy for the treatment of hypogonadal symptoms in men with total testosterone> 300 ng/dL. International braz j urol, 45(5), pp.1008-1012.
- Lee, J.A. and Ramasamy, R., 2018. Indications for the use of human chorionic gonadotropic hormone for the management of infertility in hypogonadal men. Translational andrology and urology, 7(Suppl 3), p.S348.
Evidence Based Research
This article has been researched and written based on scientific evidence and fact sheets that have then been crossed checked by our team of doctors and subject matter experts.
References, sources and studies used alongside our own in-house research have been cited below, most of which contain external clickable links to reviewed scientific paper that contain date stamped evidence.
Our team of healthcare experts and GMC registered doctors are licensed to UK GMC standards. We strive to provide you with the latest evidence based, researched articles that are unbiased, honest and provide you with accurate insights, statistics and helpful information on the discussed topic to ensure you gain a better understanding of the subject. You can read more about our Editorial Process by clicking here.
We value your feedback on our articles, if you have a well-researched paper you would like to share with us please contact us.
Quick Low Testosterone Test
If you know your total testosterone reading from a previous blood test input the results to the left above to see if your testosterone levels are normal.
Low Testosterone Levels
You may have low testosterone depending on the symptoms you have, please contact us to find out how we can help.
Please Retry
The Total Testosterone Level You Entered Is Incorrect. Figure Must be in nmol/L you can use our converter here.
Normal Testosterone Levels
Your testosterone levels appear to be in the normal range.
LOOKING GOOD!
You must be over 38, have had your ovaries removed or have suffered with premature menopause to warrant further hormone tests.
Further investigation needed
Please contact us to discuss your hormones, we need your total testosterone levels to validate your hormone deficiency. You can order a blood test here.
Low Testosterone Levels
You may have low testosterone depending on the symptoms you have, please contact us to find out how we can help.
High Testosterone Levels
You appear to have higher than normal testosterone levels, please contact us for further investigation.
Normal Testosterone Levels
You appear to have normal testosterone levels. Contact us if you have any concerns.
About the Author: Mike Kocsis
 Mike Kocsis has an MBA with a focus on healthcare administration and is an entrepreneur and medical case manager for Balance My Hormones which offers medical services in the UK and Europe. Mike has over 25 years of experience in the healthcare sector, much of that working with people who have hormone imbalances. Mike has appeared on podcasts and radio and is an expert speaker on the subject of hormone imbalance. He specialises in Testosterone Replacement Therapy and Hormone Replacement Therapy (HRT) and with his first-hand experience he has helped thousands of people suffering from low testosterone recover and regain control of their lives. You can follow him on LinkedIn and on the Balance My Hormones YouTube Channel.
Mike Kocsis has an MBA with a focus on healthcare administration and is an entrepreneur and medical case manager for Balance My Hormones which offers medical services in the UK and Europe. Mike has over 25 years of experience in the healthcare sector, much of that working with people who have hormone imbalances. Mike has appeared on podcasts and radio and is an expert speaker on the subject of hormone imbalance. He specialises in Testosterone Replacement Therapy and Hormone Replacement Therapy (HRT) and with his first-hand experience he has helped thousands of people suffering from low testosterone recover and regain control of their lives. You can follow him on LinkedIn and on the Balance My Hormones YouTube Channel.
Last update: May 2nd, 2025